
Lithium & Painkiller Safety Checker
Acetaminophen
Increases Lithium Levels by Less Than 5%
What This Means
Acetaminophen does not interfere with renal prostaglandins. It does not cause kidney vessels to constrict, meaning your kidneys continue to filter lithium effectively. It is widely considered the gold standard for pain relief for bipolar patients.
Clinical Guidelines
- Safe for regular use while on Lithium.
- Max dose usually capped at 3g/day to protect liver.
- No extra Lithium monitoring required due to this drug specifically.
Painkillers and mood stabilizers sound like a standard part of healthcare, but putting certain ones together creates a silent threat. Many people living with bipolar disorder rely on Lithiuma first-line maintenance therapy for bipolar disorder approved by the FDA in 1970 to manage their condition. At the same time, millions turn to NSAIDsnon-steroidal anti-inflammatory drugs commonly used for pain and inflammation management for headaches, arthritis, or injuries. The problem isn't obvious until it's too late. Mixing these two classes of medication significantly raises the risk of Nephrotoxicitykidney damage resulting from chemical injury and severe systemic toxicity. Recent data suggests that combining these drugs reduces the body's ability to clear lithium from the blood by as much as 60%, turning a stable treatment plan into a medical emergency within days.
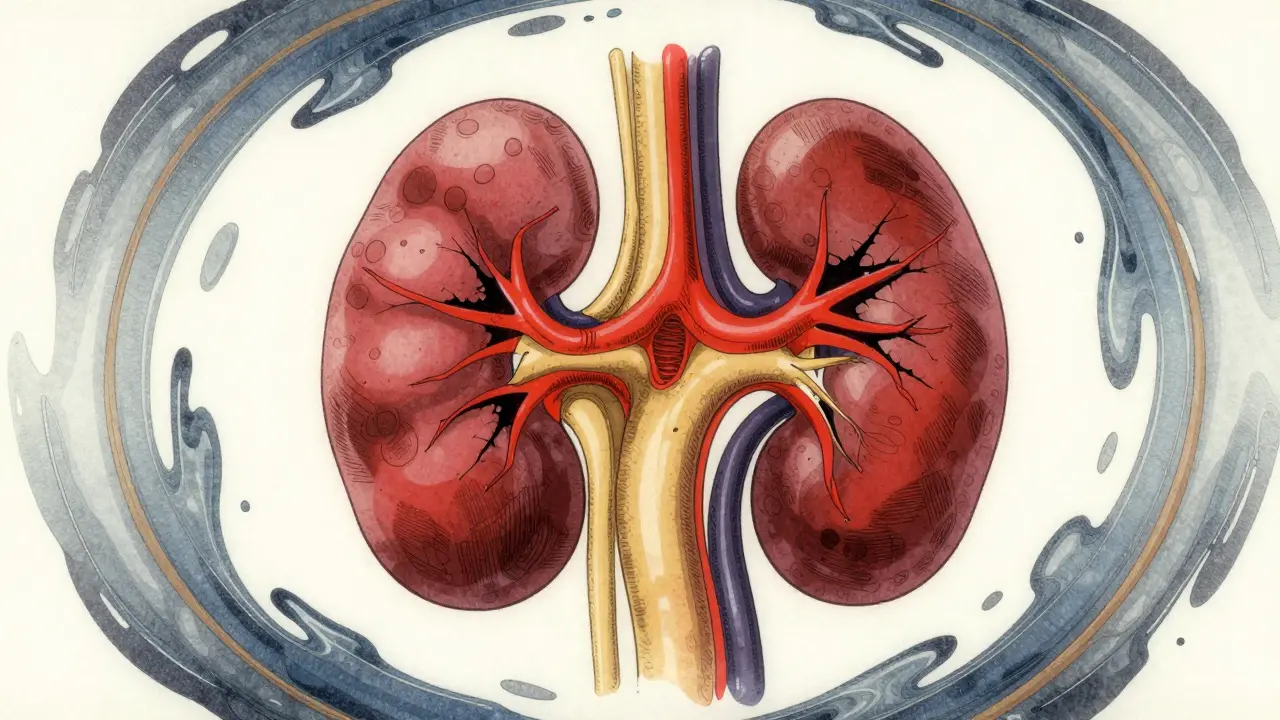
The Hidden Mechanics of Kidney Clearance
To understand why this happens, we have to look at how your kidneys work as filters. Your kidneys naturally excrete lithium through a process called glomerular filtration. However, this process relies heavily on chemicals called Prostaglandinslipid compounds that regulate blood flow in the kidneys. These compounds keep the vessels inside your kidneys dilated, ensuring blood flows freely so waste products-like lithium-can be washed out. When you take NSAIDs, they block the enzymes known as COX-2 that produce these prostaglandins. Without enough prostaglandins, the blood vessels constrict. Less blood flow means less filtering. Suddenly, the lithium meant for your brain stays trapped in your system, accumulating to toxic levels.
This isn't just a theoretical issue. Clinical studies published in journals like the Journal of Clinical Psychopharmacology document that lithium clearance can drop by 25% to 60% within 48 hours of starting an NSAID. That reduction happens regardless of whether the painkiller comes in pill form or liquid. For a patient already balancing on the edge of therapeutic efficacy, this shift moves serum lithium levels from safe zones into the danger zone where confusion, tremors, and coma become real possibilities. The kidneys, designed to filter toxins, end up struggling under the double burden of reduced perfusion and high lithium concentrations.
Which Painkillers Are the Most Dangerous?
Not all NSAIDs carry the exact same weight of risk, though caution applies to the entire group. If you are prescribed lithium, knowing the difference between specific medications can save you from hospitalization. The severity of the interaction varies depending on the chemical structure of the drug. Indomethacin stands out as the most aggressive offender. Research indicates indomethacin can spike serum lithium levels by 40% to 60%. Piroxicam follows closely, causing increases of roughly 25% to 35%. Even the most common over-the-counter option, ibuprofen, is not harmless; it typically raises lithium levels by 20% to 30%.
Conversely, some options show significantly less interaction. Aspirin and celecoxib tend to cause minimal retention, usually increasing levels by less than 10%. However, calling them "safe" is misleading. Even a 10% increase can push a patient near the upper limit of their dosage cap into toxicity territory. A comparison helps visualize the risk landscape clearly:
| Medication Class | Estimated Lithium Level Increase | Risk Category |
|---|---|---|
| Indomethacin | 40% - 60% | Very High |
| Piroxicam | 25% - 35% | High |
| Ibuprofen | 20% - 30% | Moderate-High |
| Celecoxib | < 10% | Low (but requires monitoring) |
| Aspirin | < 10% | Low (but requires monitoring) |
Despite this variation, experts generally recommend avoiding all NSAIDs while on lithium whenever possible. The variability in individual metabolism means what is low-risk for one person could trigger acute kidney injury in another, especially in older adults whose renal function has naturally declined with age.
The Synergistic Threat to Kidney Health
Beyond the immediate spike in lithium toxicity, there is a longer-term concern involving permanent kidney damage. This is what doctors refer to as chronic kidney disease progression. Lithium itself poses a mild risk to renal health over decades due to its direct effect on glycogen synthase kinase 3 beta in principal cells. However, adding NSAIDs accelerates this damage exponentially. The combination creates a dual pathway of injury: the drug inhibits essential cell repair mechanisms while the NSAID restricts the blood supply needed for survival.
Data from a large cohort study in JAMA Network Open highlights the magnitude of this risk. Patients using both lithium and NSAIDs faced a 3.2-fold higher risk of acute kidney injury compared to those taking lithium alone. The danger window is particularly narrow and sharp; the highest risk occurs within the first 30 days of starting the pain medication. Furthermore, a longitudinal analysis showed that users of this combination experienced a 2.8-fold higher rate of significant decline in kidney function (specifically eGFR dropping by more than 30%) over five years. This suggests that repeated short courses of NSAIDs aren't just temporary annoyances-they are cumulative insults to the organ system handling your medication.
Safer Alternatives for Pain Management
If you cannot skip pain relief entirely, switching to alternative analgesics is the safest route. AcetaminophenA non-opioid analgesic and antipyretic drug, widely known by brand names like Tylenol or Paracetamol, does not interfere with lithium excretion. Studies confirm it causes less than a 5% change in lithium levels, making it the gold standard for first-line therapy in this population. Guidelines from organizations like CANMAT explicitly recommend capping acetaminophen doses at 3 grams per day to avoid liver stress, but within that limit, it remains chemically compatible.
For moderate to severe pain where acetaminophen isn't enough, opioids like tramadol offer a middle ground. While they require caution due to potential dehydration effects that could indirectly lower kidney flow, they do not block prostaglandin synthesis directly. Starting low (25mg daily) allows the body to adapt. Another option is topical NSAIDs, such as creams or gels applied directly to painful joints. Because absorption into the bloodstream is minimal compared to oral tablets, the systemic impact on kidney function is drastically reduced. Always discuss these swaps with your psychiatrist or GP before changing your regimen.
Protocols for When Mixing Is Unavoidable
Sometimes, clinical necessity demands short-term NSAID use-for instance, during recovery from surgery. In these cases, strict monitoring becomes non-negotiable. The American Society of Nephrology advises that if co-prescribing is absolutely necessary, you must monitor lithium levels twice a week. Weekly checks of renal function are required for the initial four weeks. Hydration is equally critical; drinking at least 3 liters of fluid daily helps maintain the glomerular filtration rate and mitigates some of the volume loss caused by the drugs.
You should expect your doctor to reduce your lithium dose by 25% to 50% upon starting an NSAID, even before blood tests confirm a rise. Waiting for bloodwork to come back positive is playing Russian roulette with your kidneys. Additionally, remember the lag effect. The interaction doesn't vanish the moment you stop the NSAID. Renal prostaglandin suppression persists for 7 to 10 days after discontinuation. Keep monitoring your levels during this washout period because your kidneys haven't fully regained their normal filtering speed yet.
Systemic Challenges in Medication Safety
A persistent hurdle in managing this risk is communication gaps between different specialists. Often, a cardiologist prescribes heartburn or pain medication without checking psychiatric records, leading to accidental exposure. Electronic health record alerts have shown promise, reducing co-prescribing errors by around 35% in large health systems, yet nearly half of providers still miss the warning. Patients act as their own final defense system. Carrying a physical medication list and explicitly stating "I take lithium, so no NSAIDs please" when visiting new clinics forces a safety check. Despite FDA boxed warnings implemented in 2021, market data shows nearly 30% of lithium users still receive annual NSAID prescriptions, indicating a massive need for patient advocacy.




Sophie Hallam
March 29, 2026 AT 11:38This information is actually quite important for people managing bipolar disorder.
Rohan Kumar
March 29, 2026 AT 23:37They want you sick so you buy more meds 😬💊🤡
Sabrina Herciu
March 31, 2026 AT 19:58The data regarding indomethacin is particularly alarming!!! It causes massive retention!!!
Philip Wynkoop
April 1, 2026 AT 07:49Good point :) Tylenol works better
Richard Kubíček
April 2, 2026 AT 23:55It really makes you think about how delicate our biological balance is. We often underestimate the connection between simple pain relief and complex neurological medication. The kidneys work silently behind the scenes to protect us from harm. When we disrupt that flow everything goes wrong very quickly. Understanding these mechanics helps us appreciate our own bodies more deeply.
Monique Ball
April 4, 2026 AT 15:06Hydration is absolutely critical during any switching period!!! People often forget that water intake changes renal clearance rates significantly. Doctors need to track every single week without exception!!! Missing even one test creates a blind spot in your safety net!! It feels overwhelming but it is necessary for survival!! Drinking three liters helps flush the system naturally!! You cannot rely on memory alone for dosages!! Written records prevent accidental toxicity spikes!! Family members should know the warning signs too!! Tremors mean action is required immediately!! Coma is the worst possible outcome we can avoid!! Education saves lives in these scenarios consistently!! Please share this with anyone taking mood stabilizers!! Safety comes before convenience every single time!! Stay vigilant and keep those logs updated!! We have tools to manage this effectively now!!! 💧📝✅
gina macabuhay
April 6, 2026 AT 12:15Patient negligence regarding medication lists is completely unacceptable behavior!
Monique Louise Hill
April 6, 2026 AT 15:09Yes! You need to take responsibility mate 😤 Don't let doctors decide for you
Austin Oguche
April 6, 2026 AT 19:29Health systems should automate these alerts better than current electronic records provide
Sarah Klingenberg
April 7, 2026 AT 03:23That would be huge :) Everyone deserves protection
Shawn Sauve
April 7, 2026 AT 16:32Keep your fluid intake high throughout the process :)
walker texaxsranger
April 7, 2026 AT 19:19glomerular filtration rate declines are ignored by clinical trial sponsors usually
Eva Maes
April 8, 2026 AT 17:12Toxic synergy is a valid concern regardless of corporate motives or hidden agendas
Debra Brigman
April 9, 2026 AT 04:15The body knows the truth before the bloodwork confirms it eventually